
{kind=link}
| Author | Affiliation |
|---|---|
| Bryan E Bledsoe, DO | University of Nevada School of Medicine, Department of Emergency Medicine, Las Vegas, Nevada |
| Matt Loptien, MD | University of Nevada School of Medicine, Department of Emergency Medicine, Las Vegas, Nevada |
| Ross P Berkeley, MD | University of Nevada School of Medicine, Department of Emergency Medicine, Las Vegas, Nevada |
ABSTRACT
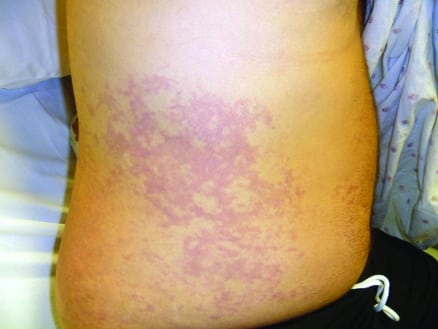
A 29-year-old man presented to the emergency department (ED) with a rash across his chest and abdomen. The rash began 2 hours before his arrival and was initially pruritic, but subsequently became painful. The patient also complained of acute onset of aching pain in both hips and his left arm. He denied associated chest pain or dyspnea, and had no paresthesias or disequilibrium. Routine laboratory studies and chest radiograph were normal. Earlier in the day, the patient had completed a dive to 235 feet in depth in Lake Mead, Nevada, but reported a very controlled ascent with appropriate decompression stops. Two days earlier, he had completed a dive to 315 feet in Lake Mead without any problems.
DIAGNOSIS
Type I Decompression Sickness
Although decompression sickness (DCS) is commonly seen in coastal regions, it is uncommon in an inland desert community. As the ambient pressure around the diver’s body decreases during ascent, inert gas (primarily nitrogen) dissolved in the blood and tissues can come out of solution and form bubbles if the rate of ascent is not well controlled with appropriate staging. The classic signs and symptoms of DCS occur as these bubbles enter and affect various body tissues. DCS is typically categorized as Type I (musculoskeletal, nonsystemic) or Type II (systemic involvement). The symptoms of Type I DCS include joint pain (the bends), cutaneous manifestations (pruritis, burning, or a marbling rash), or, less commonly, lymphatic involvement with painless edema. Type II DCS is characterized by neurologic symptoms (numbness, paraesthesias, progressing to motor weakness), vestibular symptoms (the staggers), and/or pulmonary symptoms (the chokes). As in this case, DCS can often occur despite taking appropriate decompression stops during ascent.1
The skin manifestation of DCS shown in the Figure (cutis marmorata) may precede the more serious Type II symptoms and should be treated with hyperbaric recompression. The patient received intravenous morphine for pain. The Hyperbaric Medicine service was consulted, and the patient underwent recompression per protocol. All signs and symptoms abated after therapy, and he was discharged home.
Footnotes
Supervising Section Editor: Sean Henderson, MD
Submission history: Submitted August 25, 2010; Accepted September 13, 2010
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.2010.9.2075
Address for Correspondence: Bryan E. Bledsoe, DO
University of Nevada School of Medicine, Department of Emergency Medicine, 901 Rancho Ln, Ste 135, Las Vegas, NV 89148
E-mail: bbledsoe@me.com
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources, and financial or management relationships that could be perceived as potential sources of bias. The authors disclosed none.
REFERENCES
1. US Navy Supervisor of Diving and United States Navy Dept. U.S. Navy Diving Manual, (SS521-AG-PRO-010, revision 6. Washington, DC: US Government Printing Office; 2008.
2. Conkin J, Pilmanis AA, Webb JT. Case descriptions and observations about cutis marmorata from hypobaric decompressions. NASA Scientific and Technical Information Web site; Available at:http://ston.jsc.nasa.gov/collections/TRS/_techrep/TP-2002-210779.pdf. Accessed July 8, 2010.
{kind=link}